Here you will learn:
- What Makes Medium-Chain Triglycerides (MCTs) Unique?
- How Do MCTs Help with Fat Loss?
- How Much MCT Oil Is Needed for Fat Loss?
- When Should You Take MCT Oil for Fat Loss?
- How to Take MCT Oil as Part of Your Routine
- Can You Take MCT Oil During Your Fasting Window?
- Summary: The Takeaways
This will describe the best way to use MCT oil to reach your fat loss goal.
If you’ve never heard of MCTs or long-chain triglycerides (LCTs), you can read about them here to get up to speed on some of the ideas below.
Check out the Summary Takeaways section to see an overview of this strategy. Then come back and grab all the details to fit it into your lifestyle.
What Makes MCTs Unique?
MCTs digest and absorb more easily than LCTs. In fact, MCTs use less methods of digestion compared to LCTs.
Common sources of LCTs include vegetable oils, cheese, nuts and meat. So MCTs are a useful source of energy for people who have problems digesting these types of foods.
One reason for this is MCTs can be absorbed as triglycerides. LCTs must be broken down into their long-chain fatty acids before they can be absorbed.
In general, MCTs also get broken down into fatty acids more quickly than LCTs do. These medium-chain fatty acids also go directly to the liver for use as energy. Long-chain fatty acids need extra packaging and transport before they can be used.
Overall, this means MCTs are generally better for rapid energy than LCTs are.
How Do MCTs Help with Fat Loss?
One small advantage of consuming MCTs is their shorter chain length gives about 10% fewer calories than LCTs. MCTs have about 8.3 calories per gram for versus 9 calories per gram for LCTs. But this does not tell the whole story.
You may normally think of foods only in terms of their calories. But MCTs have some other interesting properties compared to LCTs besides just calorie counts.
As mentioned above, MCTs have several unique properties compared to LCTs:
- More direct transport to the liver
- Better conversion to ketones
- More thermogenesis (body heat generation)
- More available as an energy source
- Better at reducing food intake at meals
Among these properties, the increase in ketones from MCTs is quite interesting for fat loss.
A recent study suggests that ketones can lower your hunger. People on ketogenic diets also feel less hungry, and their high ketone levels are thought to explain why.
Surprisingly, people eating very low-calorie diets (~500 kcal per day) for several weeks also feel less hungry. These people are at a level of ketosis of ~0.5 mM beta-hydroxybutyrate (BHB; one of the ketone bodies) which you can also reach just by taking MCTs.
This ability of MCTs to increase ketones may help explain why MCTs reduce food intake better than LCTs.
So from here on, this property of MCT oils will be the focus for using MCT oil as a fat loss tool. The goal is to keep ketones high throughout the day, and especially before meals, to help make meals smaller or skip meals altogether.
What Type of MCT Is Best for Fat Loss?
Most studies use MCT oils which contain a mixture of MCTs. And while these do work to help reduce food intake, they don’t maximize ketones.
The goal is to use the smallest amount of MCT oil to get the biggest boost in ketone levels.
As explained here, MCTs are made of fatty acids which are 6-12 carbons long. MCT oil mixtures contain up to 55% C8 MCTs and 35% C10 MCTs, though some MCT oil products have lower percentages of each. Most MCTs in coconut oil are C12 MCTs.
As Figure 1 below shows, C8 MCT oil is more ketogenic than coconut oil or mixed MCT oil.
Figure 1: C8 MCT oil increases total ketones more than mixed MCT oil or coconut oil. 4- to 8-hour area under the curve values (20 mL taken 4 hours post-meal) adapted from Vandenberghe, et al. 2017.
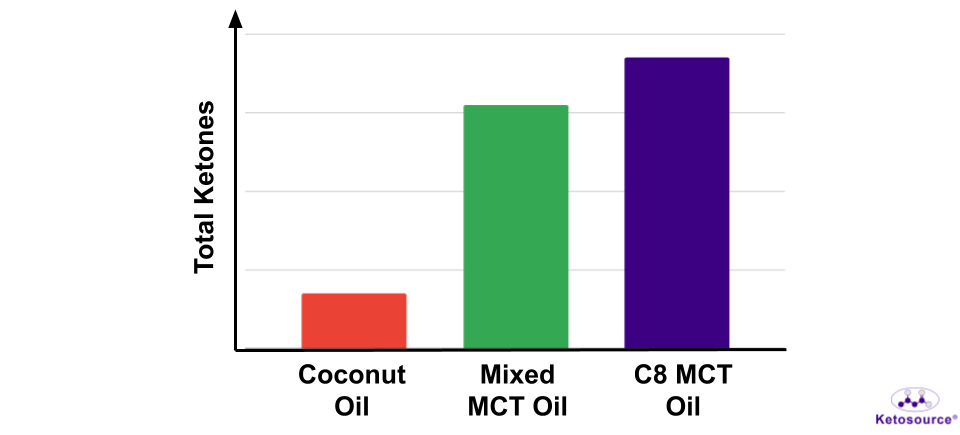
These oils all contain calories (~150 kcal per 18 mL tablespoon), so C8 MCT oil will give the highest ketone boost per calorie.
This makes C8 MCT oil better to use for fat loss than other MCT oils like mixed MCT oils or coconut oil.
How Much MCT Oil Is Needed for Fat Loss?
The best amount per individual is not known. The research has not agreed on how much MCT oil is best for fat loss.
The amount of MCT oil per day used in the research for fat loss varies widely from half a teaspoon all the way up to 3 tablespoons (approx. 2 – 54 mL) per day. The durations of the studies also vary from 4 to 16 weeks. And some studies used different amounts for women and for men.
These studies also involve swapping out foods for MCTs. While some people may find this easy to do, it requires some effort to swap out ~150 kcal food for one tablespoon of MCT oil. It’s just not practical for most people.
More importantly, few studies include timing as part of their protocol. Timing of the MCT oil dose is important for a couple of reasons.
Specifically, timing a dose before a meal gets ketones high for that meal. This is likely to keep hunger down at that meal and help you eat less without feeling deprived.
Timing a dose so that it’s not taken with lots of food (especially carbohydrates) is important as well. This ensures that you get maximum ketone levels from the oil.
So, what is the best way to dose the MCT oil?
As mentioned earlier, studies have found that people on very low-calorie diets are not hungry when their BHB level is ~0.5 mM. One study showed that hunger comes back as BHB drops from ~0.4 mM down to ~0.1 mM.
However, these studies involve calorie restriction, and MCT oils may not mimic all that comes with calorie restriction. Calorie restriction may affect hunger in more ways than MCT oils.
But ketones can lower hunger and appetite by themselves, so these studies do provide some reasonable BHB targets to aim for when dosing MCT oil, even if it has not been directly tested yet in the research.
So you want a dose that will boost your BHB higher than 0.12 mM. Ideally, you should aim for a boost of 0.5 mM BHB from MCT oil.
You can test your blood with a blood ketone meter to see what dose works for you. But one tablespoon of MCT oil will certainly do this, especially if it is C8 MCT oil. So you do not need to take more than one tablespoon of MCT oil at a time for the best results.
What About Stomach Problems?
The MCT oil can give people stomach problems (e.g. nausea and diarrhoea), especially when they first start taking it. So eating a small snack (e.g. a high-fiber snack such as avocado) with the oil is okay if this helps with stomach issues. But you should avoid taking the oil with a large meal in order to maximize your ketones from the oil.
If you have general stomach issues, try an MCT powder made with acacia fibre. This will be more gentle on your stomach and make the oil easier to take.
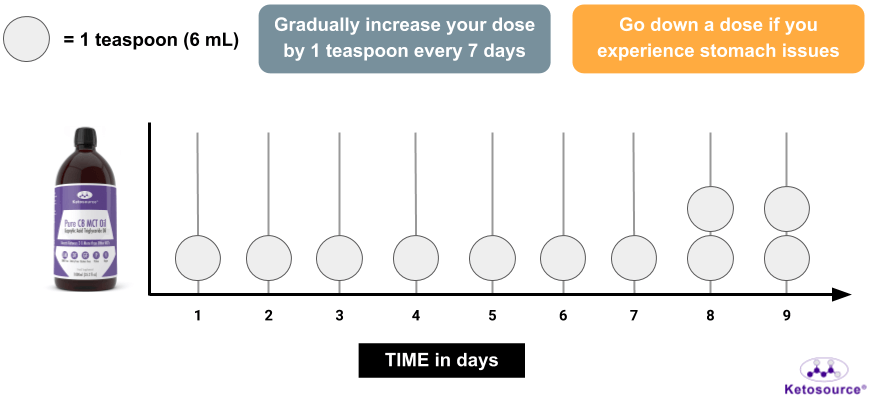
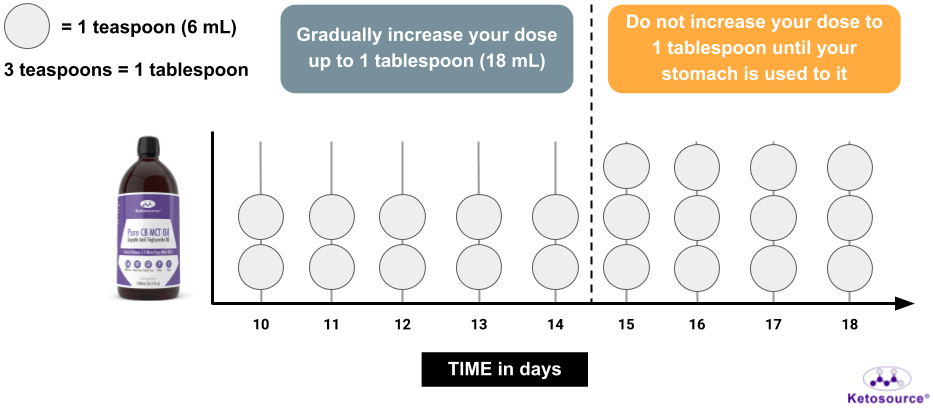
Otherwise, you should start slowly by taking just 1 teaspoon of MCT oil at a time. You should then gradually work up to 1 tablespoon as illustrated in Figure 2 below.
Figure 2: How to adjust to MCT oil over time.
When Should You Take MCT Oil for Fat Loss?
In many of the studies on MCT oil and fat loss, MCT oil is taken as part of a food or meal. In other studies, the exact MCT oil protocol is vague. They only show how much MCT oil was consumed per day.
Taking MCT oil alone before a meal raises ketones more than taking it with a meal. And internal Ketosource consulting data shows that people do best when taking MCT oil at least an hour before a meal.
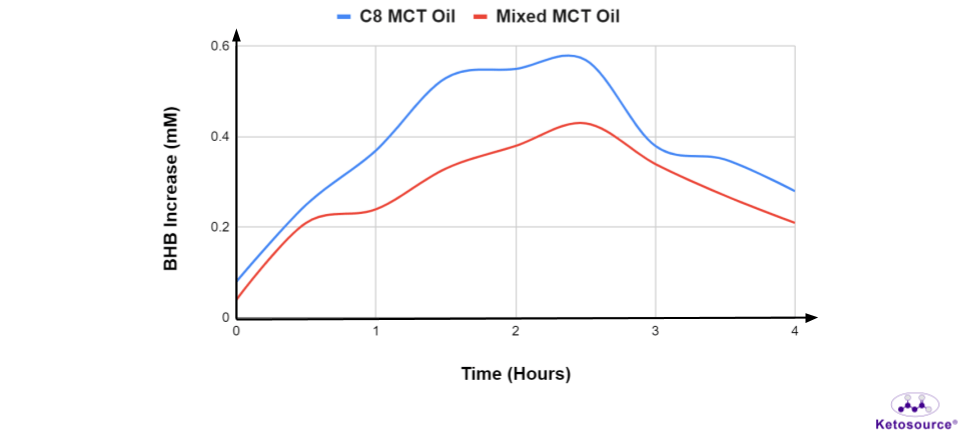
As Figure 3 shows below, 20 mL (about one tablespoon) of mixed MCT oil can raise BHB by ~0.2 mM within an hour of taking it. As mentioned above, this is in the 0.1-0.5 mM boost you should aim for before a meal.
Figure 3: The rise in ketones after taking 20 mL mixed MCT oil or C8 MCT oil four hours after a meal. Graph adapted from St-Pierre, et al. 2019.
So MCT oil should be taken by itself or with a small snack at least an hour before a meal. This will get ketone levels high before the meal and help you eat less at that meal.
Taking MCT Oil Throughout the Day
The length of time MCT oil raises blood ketones is important when considering dosing frequency. As Figure 3 shows above, ketones reach their peak around 1.5 to 2.5 hours after taking MCT oil. Then they drop from 2.5 hours onwards.
Ketones stay high for at least four hours after taking MCT oil. So there should be four hours or more between doses of the MCT oil.
In the Morning and Early Afternoon (Up to Two Doses)
Taking MCT oil with breakfast can reduce food intake for the day. So the early morning is the best time to take MCT oil. And ideally you should take it at least an hour before breakfast to maximize ketones (e.g. on waking).
Then you should take another dose of MCT oil later in the morning/ early afternoon at least an hour before your 2nd meal.
If you do not eat breakfast or if you follow time-restricted feeding, then take the oil at least an hour before your first meal. This will help you reduce the size of your first meal or even skip it. And you do not need to worry about the oil breaking your fast, as discussed below.
In the Late Afternoon (One Dose If Needed)
This is an extra dose if you really need to combat hunger or prepare for your evening meal. MCT oil contains 155 kcal per 18-mL tablespoon (1 teaspoon ~ 50 kcal), so taking more isn’t always better if your goal is fat loss.
If you are going to take MCT in the afternoon, you should take it before 4 PM. This is because it can interfere with sleep (possibly from thermogenesis).
In the Evening (Avoid)
As mentioned above, taking MCT oil too late in the day can cause trouble with sleep.
Taking MCT oil throughout the day should help to prevent overeating at night. But if you eat your evening meal past 7 PM, or if can’t control late night snacking, you could take MCT oil in the evening at least an hour before your last meal.
Total Amount of MCT Oil per Day (Summary)
The range to aim for is 1-3 doses of MCT oil per day. Since each dose should be no more than one tablespoon, this means you should take no more than three tablespoons of MCT oil per day for fat loss.
The goal is to use the least amount of MCT oil needed to help you eat less throughout the day. So don’t take a dose of MCT oil if it’s not specifically to help you reduce a meal’s size or skip a meal.
How to Take MCT Oil as Part of Your Routine
The most important aspect of MCT oil is taking it at the right time. So you need to plan ahead and make sure to take MCT oil consistently.
Use Table 1 below to see how MCT oil can fit into your eating routine.
Table 1. Methods for fitting MCT oil into your eating routine.
| Black Coffee | Yes | Try an MCT creamer if you like your coffee creamy. |
| Black Coffee With Butter (Bulletproof) | No | Butter will increase your calorie intake without helping you eat less at your next meal. It is also easy to drink too many of calories like this without realizing it. So these high-calorie drinks should be avoided when your goal is fat loss. |
| Tea (Plain) | Yes | Same as coffee. Try an MCT creamer if you normally add milk to your tea. |
| Cooking | No | MCTs burn at low cooking temperatures (160 degrees C). |
| Toppings/ Dressings | Maybe | Taking MCT oil with a meal won’t help you eat less at that meal. It will also blunt the increase in ketones from the oil. And you risk losing most of the oil or not getting the appropriate dose as it will drain onto your plate. |
| Smoothies | No | A smoothie will block the oil from turning into ketones. Liquid meals like this often leave you hungry as well. |
| Straight | Yes | The oil has little taste or odor. |
Can You Take MCT Oil During Your Fasting Window?
Intermittent fasting methods (e.g. time-restricted feeding and alternate-day fasting) often have strict eating windows. Sometimes the hunger can be overwhelming and make you want to give up, especially if you are just getting used to it.
As described in the Ketosource article on fasting, fats like MCT oil do not hurt your fasting benefits very much. So, if you need something to help you get through a difficult part of your fast, some amount of fat is okay to take.
You can take up to one tablespoon of the oil by itself without worry. And if you need to take a second dose on the same day, just make sure it’s six hours after the first. This extra time is to make sure it doesn’t interfere with your growth hormone, which helps you burn fat during fasting.
The most important part of intermittent fasting is consistency. So do not worry if you need to take MCT oil sometimes in order to stay consistent.
Summary: The Takeaways
To get the best fat loss results, you should take MCT oil based on your normal eating schedule and your stomach tolerance.
Takeaways: How to Achieve Your Fat Loss Goal
- Start with a low dose if you’ve never used MCT oil before
- Start with a teaspoon as your dose, then steadily increase up to one tablespoon over a few weeks
- Use MCT powder which has acacia powder if you have general stomach issues
- Take a dose of MCT oil at least an hour before a meal to help you eat less or skip the meal
- You want a ketone boost of 0.1-0.5 mM by the time you eat
- Avoid taking MCT oil with too much food (especially carbohydrates) as this dulls the effect
- Do not take more than 1 tablespoon per dose
- Aim for 2 doses of MCT oil per day or less
- A morning dose is the most important if you eat breakfast
- If you skip breakfast or follow time-restricted feeding, take your first dose before your first meal of the day
- Avoid taking the oil past 4 PM unless you eat late at night
- MCT oil is safe for fasting
- Take up to one tablespoon of the oil at a time to help with hunger
- Spread your doses out by six hours or more during fasting to promote fat burning